Methods and findings of a multi-day performance research lab that evaluated the efficacy of a novel nerve sensor in the context of a physically inclusive performance practice.
Making the musical performance more accessible is something that many artists, such as Atau Tanaka and Laetitia Sonami, as well as scientists, have been aiming for a while. Therefore many efforts go toward the “nerve-sensor” direction. With this kind of approach, the detection of signals from nerve fring is more likely to happen rather than the skeletal muscle movement, so performers with physical conditions have more control over the sensors.
Even though the variety of gestures wasn’t as broad as other gestural instruments offer, the affordance of communication of gestural effort was better as proved in the explorations made on different sound-practices like free improvisation and the development of a piece called Frustentions.
Thanks to the Electromyography, a technique used to measure the electrical activity of skeletal muscles and nerves through the use of non-invasive sensors placed directly on the skin, we have seen more and more people with muscle atrophy or compromised volitional control of skeletal muscles, having access to technologies, for example when it comes to gaming. But, as it usually happens, the broader the accessibility is the more potentially harmful lens can come with it. Therefore it is important to keep in mind that every individual is unique and be aware of the invisible boundaries that the technology can set around the people it’s supposed to serve.
The more people with different physical and mental abilities get involved in these sound-making explorations, the better and opener accessible the design of the interfaces will be.
For this specific exploration, there were 4 investigated parameters: sensor position, gesture types, minimal-movement gestures, as well as various sound-mapping parameters. The lab was structured into several sessions, each concluding with a performative exploration, as well as a structured public showcase and discussion at the end of the lab. Other research lines like minimal-movement “neural” gestures were also investigated but not much data could be gathered. The outcome of the session was the previous said composed piece: Frustentions. A fixed media composition developed during the workshop.
Three groups of gestures were determined during the sessions in order to record the needed data: Effort gestures, which were particularly suited to audio effects that are well-aligned to swelling such as distortion, delay, or reverb, and adjustment gestures, which often required full focus and were not necessarily accessible at all times during a performance; and trigger gestures.
The nerve sensor was compared with other interfaces like the MiMu glove, the Gestrument, and Soundbeam. Even though these other instruments allowed wider recognition of the number of gestures with better accuracy, it was more challenging to use with limited fine-motor capabilities. In addition, the wearable sensor afforded the performer greater opportunities to connect visually with ensemble members or the audience as there was no immediate requirement to view or interact directly with a screen.
Conclusions
Research aimed at making musical performance accessible to everyone is something that has multiple benefits, clearly on a physical level, but above all on a neural and psychological level. It is surprising how many things associated with leisure are out of reach for many people, simply because their physical condition does not meet the standards for which they are designed. The possibility that all these people can access activities of enjoyment represents a clear increase in the quality of life for them and for the people around them.
Nerve sensors are just one example, and thanks to this exploratory initiative we can get to know them and compare data with other instruments on the market. In more advanced stages of research, I would like to imagine that these interfaces are also used medically, to alleviate the effects of some diseases, improve physical conditions, and even reduce motor damage that originates in the brain by promoting nerve and muscle movement. Music is obviously a means of enjoyment, but together with science, it can be a means of healing.
Radiology is the discipline that is responsible for deciphering the information contained in images of our body to diagnoseor inform other specialists and even the patients themselves of how the pathologies suffered are developing.
Radiologists are exposed to a workload of approximately 200 cases in a normal working day. 200 cases equal 200 people, with different illnesses, and different stories. With this workload, the person’s story is normally relegated to the background, but we all know that human closeness in a context like this is a necessary asset and it should always remain in the foreground.
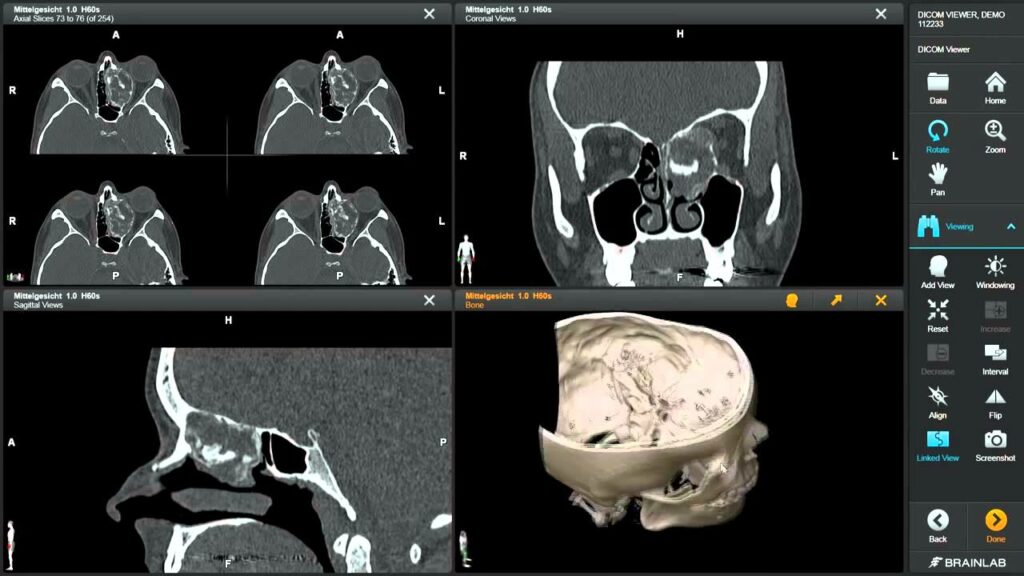
There are different software tools, as well as imaging standards, that radiologists use to do their work. Among them, we could speak of DICOM (Digital Imaging and Communication in Medicine), the standard for the communication of information related to images. Regarding software, we could talk about PACSonWEB, a portal where both hospital specialists or doctors from private practice, and patients themselves can easily access their image repositories, avoiding the bureaucracy and long waits involved in transferring from one source to another.
Companies from all over the world are dedicated to the development and improvement of these systems, trying to reduce as much as possible the time that specialists spend examining each image so that they can dedicate that time to their own professional well-being or to dealing directly with patients, procuring that necessary human proximity for a longer time.
How can design help in this specific specialty? Through the interfaces and the constant study of the behavior of professionals in the work context. The interfaces with which doctors interact daily should be clear and accessible, all the most used tools should be quickly identifiable and above all, the series of images should be able to be combined in the way that is necessary to obtain a 360 view. degrees of the pathology being analyzed. It must be taken into account that these people spend the day in a dark room, therefore, the interfaces must be designed so as not to overexpose the eyes of the professionals. Likewise, it is at that very moment of image analysis in that dark room when the diagnosis is made, not afterward. Typing would be a waste of time, therefore the design and development of dictation tools and good speech recognition are highly necessary.
To sum up, the continuous interaction with radiology professionals to understand their needs and how they work, the design and conception of interfaces in which navigation is totally intuitive, and the reinforcement of tools that facilitate voice interaction within the software, are the steps that the UX Design and UI Design must imminently address in order to improve the quality of life of radiologists in their work environment.
In the course of my visit to Spain during the Easter holidays, I had the opportunity to have a short interview with one of the heads of the cardiology department of the Salamanca general hospital.
After listening to what the doctor told me, 3 things were clear to me:
The time spent on correcting minor technical errors or sharing information between specialists should be reduced to the maximum in order to be able to use it in dealing directly with patients.
Advances in technology are very effective, but we cannot forget that the main customers of health systems are the elderly people, and this is going to be the tendency at least in the near future.
Pedagogy is key in order to making patients stop seeing the hospital as a hostile environment. Time and tools are needed to provide this inclusion prior to treatment and, if possible, the availability of real people for those who do not feel so comfortable with virtual assistants.
Here is the full interview.
*This interview has been the first instance recorded in Spanish and afterward translated and transcripted to this document.
Me: Hello! Thank you for taking some time for me, I know you have probably a very packed day.
C: Yes, indeed. But no problem at all, thank you for coming.
Me: My pleasure. Just a little information before we jump into the interview itself: This interview is for educational use. I want my master’s thesis to be related to healthcare, more specifically speaking I want to find out what are the design challenges healthcare is facing right now. Since healthcare is just a big umbrella that brings together many different disciplines, I have decided to delve into radiology. I think it is a field where many different types of software and hardware are used, and also there is an ongoing relationship with other specialists and patients if I am not mistaken. All of this makes the field very attractive for a designer, and that’s why I’m here.
The information will be shared in a blog that students and teachers from my department can access as well as will be used to shape the final version of my master thesis. Only if you consent, I’ll use some of the comments made during this session as quotes within the master thesis, only then, by using the proper form of citation. And here ends the bureaucracy.
C: hahaha! No problem, of course, you can use the information for your master thesis and I’ll be happy to be quoted within it. So go ahead!
Me: Thank you so much. Let’s start then.
Me: How long have you been working here?
C: 15 years already!
Me: That is time enough to gather many different experiences. Tell me a bit about your daily routine. How many patients do you see on a normal day?
C: 15 to 30. Depending on the pathologies. Sometimes I meet on the same day with patients who are going through similar pathologies because it is easier for me to do a bit of pedagogy with them and also to easily access the repositories. There is a huge archive where all heart diseases are collected, and they are labeled in alphabetical order by the name of the pathology. Therefore, I spend less time looking for a specific record if I move around the same area all the time. But of course, I always give priority to urgent issues, and you never know when a new one is going to show up during your day.
Me: Besides meeting your patients, do you have other important meetings that you have to attend in your day?
C: Other cardiologists. Residents. Specialists from many different fields, like, for example, radiologists. We compare diagnoses, we talk about further steps within a patient’s treatment… Nurses, and sometimes administrative staff.
Me: Between all of those meetings, do you have time to take a break every now ad then?
C: Hmmm… I guess I do have breaks, but not really as many as I’d need. Sometimes I don’t have time to eat properly or I can’t take the time to clear my mind after giving bad news to a patient. Although we are used to dealing with bad scenarios and informing patients about them, in the end we are all human beings, so it is also a human need to have a space to digest that you “hurt” someone’s feelings before going on with your day.
Me: I understand. The breaks are not only to have a physical rest but also to recompose yourself psychologically.
Me: Is there something you think that will make you have more of that time you are seeking?
C: Hay muchas veces que las reuniones se podrían hacer más rápido. Algunos trámites administrativos podrían hacerse más rápido. La transferencia de datos de médico a médico para un diagnóstico posterior debería ser más rápida. Incluso hay ocasiones en las que tenemos que repetir procedimientos por falta de instrucciones dadas al paciente, o alguna pérdida de información. Son cosas que no deberían estar pasando en un gran hospital como este, porque si hay algo que buscamos, en realidad, todos buscan, es tiempo.
Me: Let’s go to the analysis of some of the devices and procedures that you daily use.
Me: What kind of devices do you use more often?
C: Cardiac ablation catheters, Cardiovascular angioplasty devices, Cardiac pacemakers, Implantable cardioverter defibrillators, Prosthetic (artificial) heart valves, Stents, Ventricular assist devices, “domestic” monitor devices, web and mobile applications or portals.
Me: Can we focus on the last ones? As I understand, patients can get more involved in those.
C: Definitely.
Me: Within the use of “domestic devices or those that patients take home, is the data collected sufficient to provide a complete diagnosis?
C: Yes and no. For many patients, it is enough because we only look for abnormalities. So we see them or we don’t. But answering your question, no. It is not enough to completely diagnose a pathology. If we find an abnormality through the monitor, we will have to perform further procedures to find the best way to proceed with that specific patient. And many of those procedures will need to be done inside the hospital.
Me: How many times do you need to repeat monitoring procedures? Average per year.
C: Around 15% of the whole amount of procedures.
Me: What do you think is the main cause?
C: Technical problems many times. But there are also times when patients don’t understand exactly what we need for them, so we have to explain again how to interact with the device, what they can do, what they can’t do, and redo the procedure.
Me: Is there a specific demographic group where the repetitions occur more often?
C: Elderly people. In reality, most cardiology patients are older people. Sometimes we have children or young people who have heart problems but… You know, we are in a very old society. And it is expected to be even greater in the coming years… Medicine has to see the elderly as its main client and adapt procedures to them. And that takes time. Exactly what we don’t have here.
Me: These elderly people, is there something they complain about when they are required to wear this device on them?
C: They feel insecure. They don’t see why they need this machine if I’m here. I’m the doctor, what a machine is going to the better than me? They have a lot of questions. Many don’t even understand the most basic things so… They feel uncomfortable, even though they have to wear the device for only one or two days.
Me: Do you think these people feel involved when dealing with these devices? Do they feel like an active part of the procedure or a secondary actor?
C: Honestly, I think they feel totally aside. They don’t know what is going on. They follow instructions. Everything is cold and aseptic. They don’t have a voice. But they do have a voice, but many times we don’t have the time to listen to them because we use all our available time discovering what is going on there.
Me: What do you think could be done in order to improve patient engagement and involvement?
C: Definitely avoid all of those technical errors that are grabbing our time for the face-to-face relationship with our patients and the pedagogy we could do with them. More time = more pedagogy = less repetition of procedures = more rate of success when finding the diseases in their early stages.
Me: What do you think has been already done to improve this?
C: Many of our applications and portals, as well as AIs, provide training to our patients previous to their procedures. We go back to the problem of getting the elderly people there. They rather speak with you than navigate an application looking for the information they need or listen to the instructions from a non-human character. This has been widely discussed among the medical staff, so the awareness is also a good point and I guess some steps will be done to address this.
Me: Thank you so much for your time. I think I have all I need. Do you maybe want to talk about something that I didn’t ask you that you would like to share with me?
C: I think I don’t have any further information I can share with you. I already talked too much! But if more questions come up to your mind, don’t hesitate in contacting me. Thank you for the interview!